Introduction
Biomedical procurement is not an administrative function. Every purchasing decision - a ventilator supplier, a PPE contract - directly affects whether patients receive safe, uninterrupted care.
The consequences of getting it wrong are concrete:
- Supply disruptions halt clinical operations mid-procedure
- Non-compliant vendors trigger FDA enforcement actions
- Gaps in vendor oversight create HIPAA exposure
- For PE-backed organizations, these failures compound pressure on margins and value creation timelines at exactly the wrong moment
This article covers what biomedical procurement transformation actually means, why the status quo carries measurable risk, the strategic pillars that drive effective change, and how to build an operating model capable of sustaining it - including how offshore capability centers are closing the domain expertise gap that leaves most mid-market healthcare organizations exposed.
Key Takeaways
- Biomedical procurement directly affects patient safety, regulatory standing, and clinical continuity - a strategic function, not an administrative one
- FDA device recall records rose from 2,260 in 2021 to 3,275 in 2024, making recall monitoring a procurement responsibility
- Transformation rests on five pillars: supplier qualification, risk monitoring, contract management, diversified sourcing, and cross-functional governance
- Mid-market and PE-backed organizations face a domain expertise gap that offshore capability centers are purpose-built to close
- Phased transformation starts with spend visibility and supplier rationalization, then scales into strategic sourcing and contract optimization
What Is Biomedical Procurement Transformation?
Biomedical procurement covers the end-to-end process of sourcing, qualifying, contracting, and managing vendors supplying medical devices, equipment, supplies, and diagnostics to healthcare organizations.
The transformation dimension is a deliberate shift - away from reactive, price-driven purchasing and toward a strategic model that connects procurement decisions to patient outcomes, regulatory compliance, and supply chain resilience.
What This Looks Like in Practice
Most healthcare procurement functions today typically include one or more of these patterns:
- Fragmented vendor records spread across departments
- Manual onboarding with inconsistent documentation standards
- Contract renewals managed by calendar reminder rather than performance data
- Compliance tracking done reactively, after an issue surfaces
Transformation replaces these patterns with structured workflows, vendor performance accountability, and data-backed decision-making across the full vendor lifecycle.
The practical goal is a procurement function resilient enough to withstand regulatory scrutiny, supply disruptions, and the performance expectations of investors and accreditation bodies - all at once.
Why Biomedical Procurement Demands a Strategic Overhaul
Regulatory and Compliance Pressures Across the Supply Chain
The regulatory environment around biomedical procurement is demanding and enforceable. FDA purchasing controls under 21 CFR 820.50 require that healthcare organizations ensure purchased products and services meet specified requirements - this includes supplier agreements, contractor quality requirements, and change-notification protocols.
The P.T. Sankei Medical Industries FDA warning letter from 2023 illustrates exactly how this plays out: the firm received enforcement action for inadequate supplier procedures, missing supplier change-notification agreements, and insufficient contractor quality controls. These are procurement governance failures, not manufacturing defects.
ISO 13485:2016 adds another layer: Clause 7.4 specifically governs purchasing controls, supplier evaluation, and verification of purchased product. For any organization supplying or procuring regulated medical devices, compliance with these frameworks is a baseline requirement.
Getting this wrong carries serious downstream consequences:
- Product recalls and clinical disruptions
- Loss of accreditation or market authorization
- Legal penalties and enforcement action
- HIPAA liability when vendors touch patient data
HHS OCR's $2.3 million CHSPSC settlement involved a business associate breach affecting over 6 million individuals. It's a direct reminder that biomedical vendor onboarding must include PHI and Business Associate Agreement review.
Supply Chain Vulnerabilities and Patient Safety Risk
Compliance risk and supply chain structural risk are two sides of the same problem. Dependence on single-source vendors for critical biomedical components creates fragility that no compliance program alone can fix. One quality incident, audit failure, or supply disruption can halt clinical operations or compromise patient safety before a response plan can be activated.
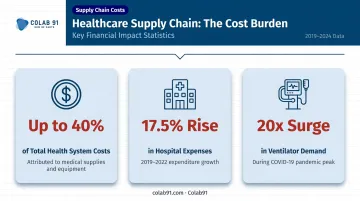
COVID-19 exposed this fragility at scale. HHS ASPE reported that ventilator demand increased 20 times during the pandemic, with nearly 90% of N95 respirators imported - primarily from China. The federal response required DPA-related procurement of 181,000 ventilators and 166.5 million respirators, with initial contracts valued at approximately $3.9 billion.
At the hospital level, the AHA reported that AHRMM vetted 800+ nontraditional suppliers during COVID, approving 300+ with vetting activity peaking at 20 to 40 vendors per day. That pace of crisis qualification reveals what happens when pre-crisis procurement playbooks don't exist.
For PE-backed and mid-market healthcare organizations, these disruptions carry financial weight beyond patient safety. Medical supplies and equipment can account for up to 40% of total health system costs according to McKinsey, with AHA data showing overall hospital expenses rose 17.5% between 2019 and 2022.
Procurement failures in this cost environment are not operational inconveniences. They are direct threats to margin performance and investor expectations.
Key Pillars of an Effective Biomedical Procurement Strategy
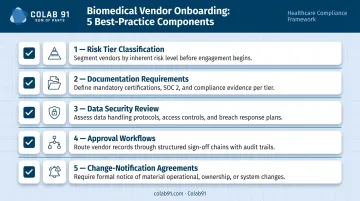
Structured Supplier Qualification and Onboarding
Vendor qualification must happen before the first purchase order. A best-practice onboarding checklist covers:
- Risk tier classification - categorize vendors by spend, clinical criticality, and regulatory exposure
- Documentation requirements - audit history, regulatory certifications, quality management system evidence, and ISO 13485 alignment where applicable
- Data security review - BAA requirements and PHI-risk assessment for any vendor with access to patient data
- Approval workflows - defined escalation paths for non-compliant vendors, not informal workarounds
- Change-notification agreements - contractual obligations for suppliers to flag product, process, or ownership changes
The P.T. Sankei enforcement action is a useful calibration point: the absence of supplier change-notification agreements was a citable deficiency. These are achievable controls - they just require deliberate process design upfront.
Continuous Risk Monitoring and Performance Tracking
Qualification is not a one-time gate. Vendor performance fluctuates as staffing changes, raw materials tighten, or quality audit cycles lapse. A supplier that passed onboarding two years ago may carry very different risk today.
Continuous monitoring should track:
- Delivery accuracy and lead time variance
- Quality incident rates and corrective action response times
- Regulatory certification status and renewal dates
- Recall activity - FDA device recall records reached 3,275 in 2024, up from 2,260 in 2021
Automated risk flags and performance dashboards let procurement teams intervene early - before a lapsed certification or unresolved corrective action reaches clinical operations. Spreadsheet-based tracking misses precisely these gaps: certification expiry dates, recall response timelines, and audit cycle lapses that accumulate quietly between manual reviews.
Data-Driven Contract Management and Renewal Strategy
Biomedical contracts require active management beyond price and delivery terms. Active contract governance includes:
- Audit rights - the contractual ability to verify supplier compliance on demand
- Service-level expectations - defined, measurable performance thresholds with consequences
- Regulatory obligations - vendor responsibilities for notification, certification, and reporting
- Renewal triggers - performance-based renewal criteria, not automatic rollovers
Data-backed contract reviews change the leverage dynamic at renewal. Teams that enter renegotiations with documented delivery failures, pricing benchmarks, and compliance gaps hold a concrete position - one that suppliers cannot dismiss or reframe.
Diversified and Redundant Sourcing
Single-source dependency for life-critical components is a structural risk, not a cost optimization. A resilient sourcing strategy includes:
- Pre-qualified alternate vendors by category, ready to activate without a crisis qualification sprint
- Dual-source agreements for high-risk items (ventilators, infusion equipment, diagnostic supplies)
- Documented backup protocols with activation triggers and lead time assumptions
The AHA noted during COVID that healthcare organizations were actively shifting from single-source to multi-source contracts. Organizations that had already pre-qualified alternates maintained supply continuity; those that hadn't spent the crisis running qualification sprints under maximum pressure. The structural work is the same either way - the timing determines the outcome.
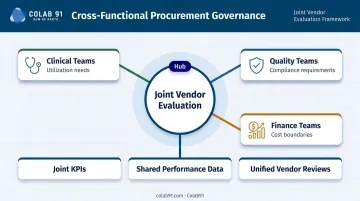
Cross-Functional Collaboration Across Clinical, Procurement, and Quality Teams
Procurement decisions in the biomedical space cannot sit with procurement alone. Clinical teams understand utilization needs. Quality teams own compliance requirements. Finance teams set cost boundaries.
Without structured coordination, procurement optimizes for the wrong variables.
Effective cross-functional governance includes:
- Joint vendor evaluation committees with clinical, quality, and procurement representation
- Shared KPIs that connect procurement performance to patient care and compliance outcomes
- Regular vendor performance reviews where all stakeholders review the same data
This structure prevents the common failure mode where procurement secures a lower-cost vendor that quality or clinical teams then reject post-contract.
Designing the Right Procurement Operating Model
Strategy without the right operating model fails at execution. A fit-for-purpose biomedical procurement operating model requires clear category ownership, defined sourcing workflows, supplier performance governance, and spend visibility infrastructure.
The Capability Gap in Mid-Market Healthcare
Mid-market and PE-backed healthcare organizations frequently run lean procurement functions - generalist teams that handle purchasing across categories without the domain expertise to manage complex regulatory requirements, run strategic sourcing events, or build supplier analytics. This is a structural problem, not a headcount problem.
Adding bodies to a generalist team does not produce domain expertise in biomedical category management, FDA compliance requirements, or spend analytics. Closing it requires a fundamentally different approach to how procurement capability is built.
The Offshore Capability Center Model
Offshore procurement capability centers augment in-house teams with dedicated domain experts in strategic sourcing, spend analytics, and category management - without the cost structure of a large onshore team.
Colab91 builds exactly this type of capability center for mid-market and PE-backed companies. The firm's "Sum of Parts" model integrates offshore expertise with the client's existing team, designed to function as a strategic hub rather than a transactional support layer. The leadership team brings over 16 years of experience scaling offshore delivery organizations, with healthcare clients including Pediatric Associates (a TPG portfolio company) and Kindred Healthcare.
Colab91's advisor Erika Jung served as Chief Procurement Officer at Pediatric Associates. That means the healthcare procurement context is embedded in the model from day one - not added as an afterthought.
Getting the Model Right Early in PE Timelines
For PE-backed portfolio companies, the window for procurement transformation is tied to value creation cycles. A well-designed operating model accelerates three things:
- Savings identification - spend visibility and benchmarking that surfaces opportunity fast
- Compliance readiness - supplier qualification frameworks that reduce regulatory exposure during hold period
- Supplier rationalization - vendor consolidation that improves pricing and reduces oversight burden
Waiting until year two or three to build this infrastructure means the highest-leverage window for cost reduction has already closed.
Technology and Spend Analytics as Transformation Enablers
Manual procurement tracking - spreadsheets, disconnected email chains, siloed contract folders - cannot meet the data demands of modern biomedical procurement. A technology-enabled procurement function looks fundamentally different:
- Centralized supplier records - single source of truth for qualification status, certifications, and audit history
- Automated compliance monitoring - alerts triggered by certification lapses, recall activity, or performance thresholds
- Real-time contract visibility - renewal dates, SLA status, and audit rights accessible without manual retrieval
- Integrated performance dashboards - cross-functional visibility into supplier health
For biomedical categories where external spend represents a material portion of total costs, analytics capabilities - benchmarking vendor pricing, identifying tail spend, flagging off-contract purchasing, and tracking savings realization - translate directly into measurable financial outcomes. Colab91's AI-powered analytics platforms are built on unified data layers that surface these insights in real time, giving procurement teams the clarity to act on what the data actually shows.
Emerging Technology Enablers
Three technology categories are worth specific attention in biomedical procurement:
- **AI for supplier risk scoring** - automated anomaly detection that flags changes in supplier financial health, audit status, or recall activity before they become operational problems
- E-procurement platforms - workflow automation for purchase orders, approvals, and contract execution that reduces cycle time and creates audit trails
- Data integration tools - connecting procurement systems with finance and clinical platforms to ensure purchasing decisions are visible to the teams that bear their consequences
Overcoming Common Procurement Transformation Challenges
Resistance to Change
Transformation programs stall when clinical and operational stakeholders see procurement as a cost-cutting exercise. Framing matters. When the internal narrative centers on patient safety, supply reliability, and compliance - rather than savings targets - procurement transformation becomes a shared goal rather than a threat.
The strongest internal advocates tend to be:
- Clinical leaders who experienced supply disruptions firsthand
- Compliance teams carrying audit exposure and regulatory accountability
Engage them early - before the program launches, not after resistance builds.
Budget and Resource Constraints
Mid-market healthcare organizations cannot always justify large upfront transformation investments. A phased approach resolves this:
- Phase 1 - Spend visibility and supplier rationalization: Low-cost, high-return activities that identify savings and reduce complexity
- Phase 2 - Strategic sourcing and contract optimization: Use Phase 1 savings to fund deeper sourcing events and contract renegotiations
- Phase 3 - Governance and analytics maturity: Build the infrastructure for sustained performance once the foundation is stable

Each phase funds the next - which matters for organizations that need to prove value before committing further resources. That proof also builds the internal confidence needed to sustain momentum into Phase 3.
Sustaining Momentum
Gains made in Phases 1 and 2 erode without a governance structure to hold them. A procurement performance governance framework includes:
- Tracked KPIs - delivery accuracy, contract compliance rates, savings realization, and category coverage
- Executive sponsorship - a senior stakeholder who owns procurement performance and can remove organizational barriers
- Regular review cadences - monthly operational reviews and quarterly strategic reviews that keep supplier performance visible at the right level
These review cadences do real work: they surface early warning signals in time to act before they escalate into clinical or financial problems.
Frequently Asked Questions
What is the procurement transformation process?
Procurement transformation is the process of moving from reactive, transactional purchasing to strategic sourcing and supplier management - It covers operating model design, process standardization, technology enablement, and capability development, typically progressing through spend visibility, sourcing optimization, and governance maturity.
What are the key components of a biomedical procurement strategy?
Five pillars define a strong biomedical procurement strategy: supplier qualification and onboarding, continuous risk monitoring, data-driven contract management, diversified sourcing, and cross-functional collaboration across clinical, procurement, and quality teams.
How does biomedical procurement transformation help reduce costs?
Transformation reduces costs through better supplier negotiation leverage, spend visibility across categories, contract compliance enforcement, and elimination of reactive or emergency purchasing behavior - which carries a price premium over planned procurement.
What role does technology play in biomedical procurement?
Technology enables spend analytics, automated risk monitoring, centralized supplier data management, and AI-driven decision support. The critical distinction is integration: procurement, finance, and clinical teams need a unified data layer they can all act on, not a collection of disconnected systems.
How should PE-backed healthcare companies approach procurement transformation?
Align transformation pace with value creation timelines - prioritize quick-win sourcing categories and spend visibility first. Use offshore capability augmentation to scale domain expertise without proportional cost increases, and ensure early savings realizations are tracked and reported against the investment thesis from the start.