Introduction
US healthcare organizations are under pressure from every direction. Hospital labor costs hit $839 billion in 2023, nearly 60% of the average hospital's total expense, while hospitals collectively spend $10 billion annually navigating prior authorizations and another $20 billion appealing claim denials.
Digital transformation has compounded the challenge: hospital spending on computing infrastructure reached $4.5 billion in 2024, up 15% year over year.
The talent required to execute on analytics, compliance, revenue cycle, and health IT doesn't come cheap onshore, and often doesn't exist in the volumes needed. That gap is what pushed large health systems toward Global Capability Centers.
Now, mid-market and PE-backed healthcare organizations - physician groups, post-acute networks, specialty practices - are catching up fast.
This article covers what healthcare GCCs actually are (and how they differ from outsourcing), which functions they handle best, how to build one strategically, and why the playbook looks fundamentally different for organizations that can't afford an 18-month setup runway.
Key Takeaways
- A GCC is a company-owned offshore team - not a vendor - giving healthcare organizations direct control over talent, IP, and institutional knowledge.
- Healthcare GCCs in India cover revenue cycle, procurement analytics, clinical data management, compliance reporting, and digital health engineering.
- GCCs can access talent at 30–50% lower cost than home markets, while expanding access to specialized skills that are scarce domestically.
- Mid-market and PE-backed organizations can build lean, high-impact GCCs without large-enterprise overhead, given the right operating model and build partner.
- HIPAA compliance is achievable offshore, but must be designed into the architecture from the start, not retrofitted after the team is running.
What Is a GCC in Healthcare - and How Is It Different from Outsourcing?
A Global Capability Center is a wholly owned, company-controlled offshore team that operates as an integrated extension of the parent organization. It is not a vendor relationship. The IP, processes, and institutional knowledge stay with the company - not with a third party whose contract expires in three years.
In healthcare, that distinction carries real operational weight. Clinical workflows handle sensitive patient data. Revenue cycle operations require deep institutional context - payer contracts, coding conventions, denial patterns - that's specific to your organization and can't be handed to a vendor who serves a dozen other clients.
Compliance functions depend on continuity. You can't rotate an outsourced team through audit preparation and expect consistent results. A GCC keeps data control, institutional context, and knowledge continuity inside the organization - where they belong.
GCC vs. GDC: A Common Point of Confusion
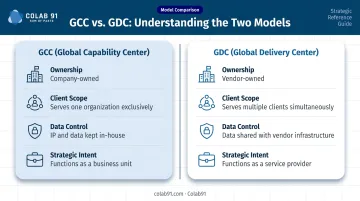
A Global Delivery Center (GDC) is typically vendor-owned and serves multiple clients simultaneously. A GCC is wholly owned by the parent company and serves only that organization. The governance structure, strategic intent, and data control are fundamentally different.
Key differences at a glance:
- Ownership: GCC is company-owned; GDC is vendor-owned
- Client scope: GCC serves one organization exclusively; GDC serves multiple clients
- Data control: GCC keeps IP and data in-house; GDC operates under shared-service agreements
- Strategic intent: GCC functions as a business unit; GDC functions as a service provider
(A quick note on the acronym: GCC also refers to the Gulf Cooperation Council, a regional political body in the Middle East. Throughout this article, GCC means Global Capability Center.)
The Maturity Curve
Healthcare GCCs started as back-office cost plays - billing support, data entry, basic reporting. That era is over. According to Zinnov and NASSCOM, India now hosts over 1,700 GCCs across all sectors, with the healthcare and life sciences segment showing strong growth driven by AI-driven diagnostics, patient-experience platforms, and regulatory technologies. There are currently 100+ dedicated healthcare GCCs operating in India, with functions spanning analytics, compliance, and increasingly AI-driven clinical applications.
Deloitte notes that GCCs have moved from resource centers to genuine centers of excellence - value creators, not just cost reducers.
Healthcare Functions Best Suited for a GCC Model
Not every function is an equally good GCC candidate. The strongest fit involves work that is high-volume, analytically intensive, rules-based, and dependent on specialized expertise that is expensive or scarce onshore.
Revenue Cycle and Billing Operations
Coding, claims processing, denial management, and payer analytics are the most established GCC use case in healthcare. The administrative burden is staggering: hospitals spend $20 billion annually appealing denials, and commercial payer payment times increased 19.7% in 2023.
A dedicated GCC team focused on denial prevention, claims accuracy, and payer analytics can attack this problem systematically - a systematic approach understaffed onshore teams rarely have capacity for.
Procurement and Supply Chain Analytics
Medical supply expense hit $146.9 billion in 2023 - roughly 10.5% of the average hospital budget. Despite the scale, procurement analytics remains one of the most underpenetrated GCC functions relative to its ROI potential.
A GCC team focused on spend analytics, contract compliance, and supplier benchmarking can surface savings opportunities that consistently go unaddressed - simply because onshore teams lack the bandwidth to run the analysis.
This is an area where Colab91's work with healthcare clients - including Pediatric Associates, the TPG portfolio company where advisor Erika Jung led enterprise-wide procurement transformation - reflects exactly this kind of analytically intensive, high-ROI function.
Clinical Data Management and Real-World Evidence
Managing clinical trial data, patient registries, and pharmacovigilance reporting requires deep analytical expertise. India has substantial talent depth here, particularly for mid-size healthcare companies that can't justify large onshore data science teams. RWE analysis is becoming central to life sciences strategy, as companies rely on it more heavily for product decisions and regulatory submissions.
Technology and Data Engineering
Building EHR integrations, population health dashboards, telehealth platforms, and AI/ML models requires continuous engineering resources. Onshore contractor markets are volatile and expensive. A GCC provides a flexible, growing engineering bench with institutional knowledge that accumulates over time - unlike contractors who turn over frequently.
Compliance and Regulatory Reporting
Audit preparation, quality documentation, and payer compliance reporting are systematizable. A dedicated GCC team can own these processes end-to-end, including:
- Maintaining audit-ready documentation on a continuous basis
- Standardizing payer compliance reporting across submission cycles
- Reducing the last-minute scramble before regulatory deadlines
Strategic Framework for Building a Healthcare GCC
Most GCCs that underdeliver don't fail for operational reasons. They fail because the strategic intent was never clearly defined before the first hire was made. Everest Group identifies lack of clear strategic intent as the primary cause of underutilized GCCs and limited perceived ROI.
The steps below address that gap directly.
Step 1: Define the Winning Aspiration
Before selecting a location or engaging a recruiter, answer one question: what is this GCC actually for?
- Cost reduction - reducing SG&A through offshore labor arbitrage
- Capability building - accessing specialized talent unavailable or cost-prohibitive domestically
- Digital acceleration - creating an engineering and analytics bench to execute transformation roadmaps
- All three - which requires explicit prioritization, because the operating model looks different for each
GCCs without a defined primary objective spread resources too thin and rarely deliver measurable ROI in year one.
Step 2: Decide Where to Play
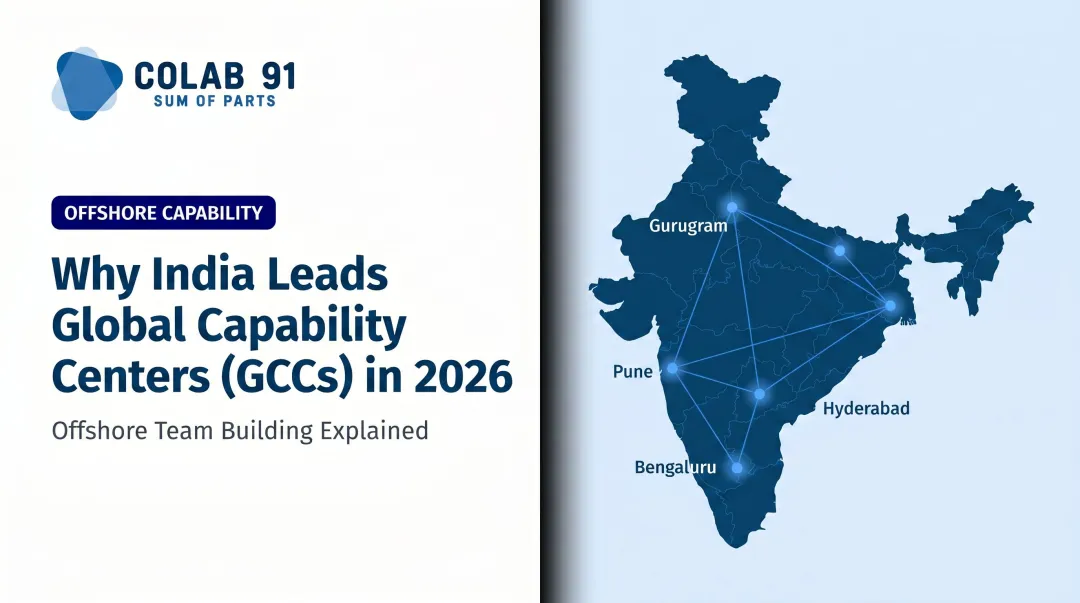
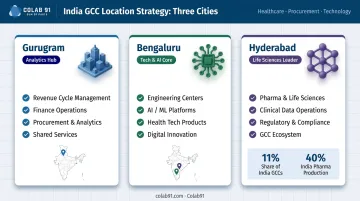
India dominates the GCC landscape. The three primary locations for healthcare-relevant GCCs are:
| City | Strongest Fit |
|---|---|
| Gurugram | Analytics, procurement, RCM, finance operations |
| Bengaluru | Engineering, AI/ML, health tech platforms |
| Hyderabad | Life sciences, pharma, clinical data, mixed functions |
Hyderabad/Telangana has emerged as a specific healthcare and life sciences GCC hub, accounting for roughly 11% of India's total GCC population and 40% of India's pharmaceutical production. Tier II locations can offer 25–30% cost advantages over Tier I cities for certain roles, though talent depth narrows for highly specialized functions.
Colab91 is based in Gurugram and builds dedicated teams for mid-market healthcare organizations specifically focused on analytics, procurement, and RCM functions - the domains where Gurugram's talent market runs deepest.
Step 3: Design the Operating Model
Three pillars determine whether a GCC actually delivers value:
- Internal org structure - hub model vs. distributed team, reporting lines, functional ownership
- Workforce planning - hiring strategy, domain expertise requirements, onboarding, retention programs
- External alliances - local HR partners, compliance advisors, infrastructure providers
Getting the operating model wrong in year one is expensive to undo. The decisions made about entity structure, IP ownership, and team composition in month one have consequences that compound across the GCC's life.
Once the operating model is set, the question shifts to how well the GCC actually connects to the parent organization. A GCC that isn't genuinely embedded in onshore workflows is just an expensive offshore team.
Governance and Integration: The Silent Failure Point
Integration requires:
- Clear reporting lines between onshore and offshore leads
- Shared KPIs aligned to business outcomes, not activity metrics
- Co-mentorship structures so institutional knowledge transfers bidirectionally
- Cultural onboarding that gives offshore teams real context - especially in healthcare, where clinical and operational nuance is everything
Governance structures only hold up if the right things are being measured. Headcount and cost savings are lagging indicators.
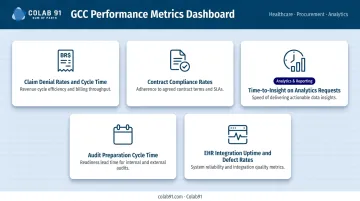
Metrics That Actually Matter
Track these instead:
- Claim denial rates and cycle time
- Contract compliance rates
- Time-to-insight on analytics requests
- Audit preparation cycle time
- EHR integration uptime and defect rates
Organizations that anchor GCC performance reviews to these metrics - rather than FTE counts - tend to see stronger executive alignment and faster course correction when gaps emerge.
Why Mid-Market and PE-Backed Healthcare Companies Need a Different Approach
Large health systems build GCCs over multiple years with dedicated PMO teams, substantial capital expenditure, and long setup runways. That model doesn't translate to a physician group with 200 locations or a post-acute care network held by a PE sponsor on a five-year value creation timeline.
The structural challenge is real:
- Setup complexity - entity formation, compliance infrastructure, and talent recruitment take time that mid-market organizations don't always have
- Capital constraints - large enterprise GCCs require upfront investment that PE-backed companies need to weigh against near-term EBITDA impact
- Lean onshore teams - mid-market healthcare companies often lack the internal bandwidth to manage a full GCC build while running the business
The PE Value Creation Angle
For PE sponsors, a well-structured GCC is a direct EBITDA lever. Offshoring SG&A-heavy functions reduces operational cost. That same offshore team can surface procurement savings and revenue cycle improvements that compressed onshore teams were never positioned to find.
As of late 2025, 610+ emerging and PE-backed enterprises have established GCCs in India - a clear signal that this model has moved well beyond large enterprise adoption. Healthcare is following.
The Colab91 "Sum of Parts" Model
The traditional GCC model asks mid-market companies to build a fully self-sufficient offshore center from scratch. Colab91's approach is different: augment in-house talent with specialized offshore domain expertise, rather than replicating the entire enterprise structure offshore.
This means a healthcare organization doesn't need to staff a 50-person GCC before seeing value. It can start with a focused procurement analytics team or an RCM denial management function - adding capability in layers as the model proves out.
Colab91's leadership team established Impendi's India operations, scaling to 100+ practitioners serving PE sponsors including Carlyle Group, TPG, Elliott, and BC Partners. Healthcare clients like Pediatric Associates (TPG portfolio) and Kindred Healthcare reflect the team's direct experience at the intersection of PE ownership and healthcare operations.
That institutional knowledge - what works, what breaks, how long things actually take - is what compresses setup risk for mid-market clients.
Compliance, Data Security, and Regulatory Considerations
HIPAA compliance for offshore teams is achievable. The architecture to make it work is well-established. The mistake organizations make is assuming it can be bolted on after the team is running - it can't.
The HIPAA Framework for Offshore Teams
The HHS requirement is straightforward: offshore teams that create, receive, maintain, or transmit protected health information (PHI) must operate under a Business Associate Agreement (BAA). Business associates are directly liable for HIPAA compliance. Subcontractors must accept the same restrictions.
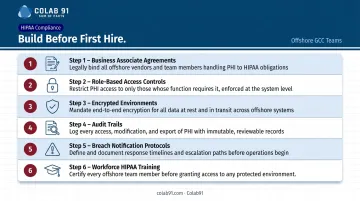
Build the compliance infrastructure before the first hire:
- Business Associate Agreements with the GCC entity and any subcontractors
- Role-based access controls limiting PHI access to those who need it
- Encrypted environments for data storage and transmission
- Audit trails tracking data access and modifications
- Breach notification protocols aligned to US reporting timelines
- Workforce training on HIPAA obligations before systems access is granted
Data residency under HIPAA is not about geography - HHS focuses on permitted use, safeguards, contracts, and breach reporting, not on whether data sits onshore or offshore. What matters is that the controls exist and are enforced.
India's DPDP Act: What Healthcare Organizations Need to Know
India's Digital Personal Data Protection (DPDP) Act was enacted in August 2023, with rules formally notified in November 2025 and an 18-month phased compliance period now underway. Healthcare organizations structuring offshore teams need to account for both frameworks simultaneously.
Key considerations when architecting data flows between US onshore teams and India-based GCC staff:
- Cross-border transfer restrictions: The DPDP Act permits India's government to restrict personal data transfers to specific countries by notification - monitor this alongside HIPAA when designing data pipelines
- Consent and processing obligations: The DPDP Act introduces data principal rights and consent requirements that layer on top of HIPAA's safeguard rules
- Dual-framework legal review: Engage advisors fluent in both frameworks before finalizing data architecture - not after the team is operational
The practical starting point is data flow mapping: document where PHI moves, who touches it, and under which regulatory framework each touchpoint falls. That map drives both your BAA structure and your DPDP compliance obligations.
Frequently Asked Questions
What does GCC stand for in healthcare?
In this context, GCC stands for Global Capability Center, a wholly owned offshore team that operates as an integrated extension of the parent organization. The same acronym also refers to the Gulf Cooperation Council, a regional political body in the Middle East - context determines which meaning applies.
What is the difference between GCC and GDC?
A Global Delivery Center (GDC) is typically owned and operated by a third-party vendor serving multiple clients. A GCC is wholly owned by the parent company and serves only that organization. That ownership structure gives the parent direct control over data, IP, process design, and talent continuity that a vendor-operated model cannot provide.
Which healthcare functions are best suited for a GCC model?
Revenue cycle management, procurement and spend analytics, compliance reporting, clinical data management, and health IT engineering deliver the highest ROI in a GCC structure. These functions are especially well-suited for organizations with high-volume, analytically intensive workloads that onshore teams lack the capacity to handle consistently.
How long does it take to set up a healthcare GCC in India?
Large enterprise GCCs typically take 12–24 months to reach full operational maturity. Mid-market organizations using an experienced build partner with established local infrastructure can have a functional team operational within 3–6 months, with meaningful output in the first year.
How do healthcare GCCs handle HIPAA compliance?
HIPAA compliance requires several controls designed into the GCC structure before the first hire: Business Associate Agreements with offshore team entities, role-based access controls, encrypted data environments, workforce training, and breach notification protocols aligned to US regulatory standards. None of these can be retrofitted after operations begin.
Can mid-market healthcare companies realistically benefit from a GCC?
Yes, and the trend is accelerating. The key is using a build model that doesn't require large-enterprise setup overhead. Starting with a focused, high-ROI function like procurement analytics or denial management, and expanding from there, allows mid-market and PE-backed healthcare organizations to prove the model before committing to full-scale buildout.