That tension doesn't get easier to manage with scale. It requires a deliberate strategy.
This guide covers the structural challenges unique to biopharma procurement, a five-pillar strategic framework, practical cost optimization levers, supplier management practices, and how to build the capability to sustain long-term value.
Key Takeaways
- Biopharma procurement is uniquely constrained by regulatory change controls, long supplier qualification cycles, and supply chain concentration risk.
- Effective strategy rests on five pillars: spend visibility, category management, compliance integration, supplier risk management, and lifecycle cost view.
- The highest-leverage cost optimization opportunities are in indirect spend consolidation and increasing "managed spend" - neither requires regulatory change controls.
- Supplier segmentation and performance tracking are operational necessities, not administrative overhead.
- Mid-market and PE-backed companies can access enterprise-grade procurement capability through offshore capability centers - without building a large in-house team.
What Makes Biopharma Procurement Uniquely Complex
Most industries can switch suppliers in weeks. Biopharma cannot.
Under 21 CFR 314.70, major post-approval NDA changes require FDA prior-approval before distribution. Moderate changes require a supplement at least 30 days before distribution.
For biologics, 21 CFR 601.12 goes further - any change to product, production process, quality controls, equipment, or facilities must be reported to the FDA, with substantial changes requiring approval before distribution occurs.
That regulatory friction makes supplier switching far more costly than in most industries. It concentrates power in existing vendors and limits competitive leverage in negotiations - which means procurement teams must qualify backup suppliers proactively, not reactively.
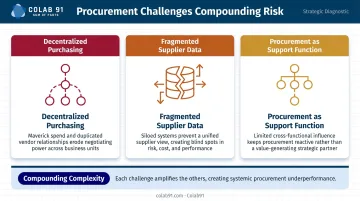
Three Structural Challenges
Beyond the regulatory dimension, biopharma procurement faces three organizational problems that compound the complexity:
- Decentralized purchasing across research, manufacturing, and clinical operations - each with different budget owners, timelines, and vendor preferences
- Fragmented supplier data sitting in disconnected ERP systems, quality systems, and spreadsheets, making enterprise-level spend analysis nearly impossible without deliberate integration
- Procurement treated as a support function rather than a strategic one - limiting its ability to influence decisions before they become costly to reverse
The FDA's FY2024 pharmaceutical quality report recorded 105 warning letters to human drug manufacturing sites - the highest in five years. Supply chain and supplier qualification failures drive a meaningful share of those. For procurement teams, that's not a background statistic - it's a direct measure of what inadequate supplier oversight costs.
Five Core Pillars of an Effective Biopharma Procurement Strategy
Pillar 1: Spend Visibility and Control
You cannot optimize what you cannot see. In biopharma, where spend is distributed across research sites, manufacturing facilities, and clinical operations, a consolidated view of spending is the prerequisite for everything else.
A mature spend visibility function includes:
- Item-level cost data across all sites and categories, not just aggregated totals by supplier
- Cross-site benchmarking to identify where the same materials are being purchased at different prices from different suppliers
- Demand forecasting that connects procurement planning to manufacturing schedules and clinical timelines
BCG's analysis of pharma TechOps procurement identifies spend visibility as the foundational capability - without it, category management, supplier negotiations, and savings programs all operate on incomplete information.
Alvarez & Marsal research points out that indirect spend as a proportion of revenue is higher in healthcare and life sciences than in any other industry - and that up to 50% of indirect savings can come from demand management alone. That opportunity is invisible without spend visibility infrastructure.
Pillar 2: Category Management
Not all spend deserves the same level of strategic attention. Category management is the discipline of segmenting spend - APIs, excipients, CRO services, indirect spend, capex - and managing each with a sourcing approach matched to its strategic value, regulatory sensitivity, and savings potential.
The practical payoff is sequencing. Categories like indirect spend and lab consumables carry no regulatory change risk and can deliver quick savings. API and critical raw materials require longer lead times for any sourcing change. Quick wins in low-risk categories fund the longer transformation work in high-complexity ones.
Category segmentation criteria for biopharma:
- Regulatory change risk if supplier changes are made
- Percentage of COGS or total spend
- Number of qualified suppliers currently available
- Demand volatility and forecast confidence
- Strategic importance to product quality or timeline
Pillar 3: Compliance and Quality Integration
GMP requirements don't run alongside the procurement process. They run through it. Under ICH Q10, companies are ultimately responsible for outsourced activities and purchased materials. That means procurement teams must have audit-ready documentation at all times, including:
- GMP certifications and site audit logs
- Corrective action records
- Approved supplier lists producible during an FDA inspection
Under 21 CFR 211.84, each lot of components must be withheld until sampled, tested, and released by quality control. Supplier certificates of analysis can only substitute for in-house testing if the manufacturer validates the supplier's COA reliability at appropriate intervals.
Compliance documentation is not a quality department task that follows procurement decisions. It must be embedded into supplier selection, onboarding, and ongoing monitoring at every stage.
Pillar 4: Supplier Risk and Relationship Management
According to McKinsey, nearly 50% of pharmaceutical executives identify sole sourcing as a primary risk factor. The U.S. State Department's 2026 medicine supply chain report adds another layer: the United States lacks manufacturing visibility for 63% of critical drugs, with China controlling 60–80% of global key starting materials for many categories. The concentration risk is structural, not incidental.
Dual-sourcing - qualifying a backup supplier for critical materials even when the primary supplier performs well - is the clearest structural mitigation. The regulatory cost of qualifying a second source is real, but it's considerably lower than the cost of a supply disruption after approval.
Supplier risk monitoring should scan for:
- Single-source dependency on geographically concentrated supply
- Supplier financial instability
- Contamination or quality failure history
- Capacity constraints relative to your demand growth
The GAO reported 102 active drug shortages as of July 2024, with shortage duration increasing despite fewer new shortages - a pattern that reflects systemic supply fragility rather than isolated incidents.
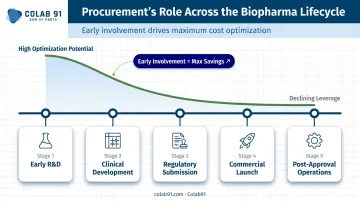
Pillar 5: Product Life Cycle Cost View
Late procurement involvement is one of the most expensive problems in biopharma. When procurement is brought in after R&D has already selected a supplier, negotiated preliminary agreements, or designed a process around specific materials, the room to optimize COGS is severely constrained.
Procurement should be involved during early-stage R&D sourcing decisions: not just to negotiate prices, but to model total cost of ownership across the product life cycle, flag single-source dependencies before they become locked in, and inform make-vs-buy decisions before they're impossible to reverse.
Downstream processing costs alone exceed 65% of biopharma production costs (BioPharm International), which means early sourcing decisions have outsized impact on long-term unit economics.
Cost Optimization Levers in Biopharma Procurement
Cost optimization in biopharma isn't a single negotiation - it requires a coordinated approach across direct spend, indirect spend, and capex. Companies that tackle all three simultaneously unlock more savings than those that work through categories sequentially.
Indirect Spend: The Highest-Leverage Starting Point
Indirect spend (facilities, lab services, logistics, maintenance, professional services, IT) is where biopharma procurement can move fastest. These categories carry no regulatory change controls, so consolidation and renegotiation don't require FDA filings or quality system updates.
The approach: aggregate enterprise-level requirements across sites, negotiate master service agreements that capture volume-based pricing, and standardize supplier lists. Alvarez & Marsal's analysis of a healthcare and life sciences company identified €10M in EBITDA improvement opportunity from indirect spend optimization alone (European case study).
Total Cost of Ownership vs. Unit Price
The cheapest API supplier is rarely the lowest-cost supplier. Quality risk, yield differences, and testing requirements change the actual economics significantly.
A cost-of-goods analysis comparing quality-assured versus non-QA API found quality-assured mifepristone API cost $7,036/kg versus roughly $875/kg for non-QA material. Yet the production cost differential for a finished combi-pack ranged from only $1.08 to $3.05 - far narrower than the raw price gap suggests.
TCO modeling should account for:
- Contamination and recall risk (the 2018 valsartan NDMA contamination originated from an API supplier's manufacturing process)
- Delivery reliability and safety stock requirements
- Regulatory qualification costs for any future changes
- Quality failure rate and associated batch write-off risk
Getting TCO decisions right depends on having the data infrastructure to compare suppliers accurately across sites and categories. That's where managed spend becomes critical.
Spend Analytics and Managed Spend
The share of total third-party spend running through centralized procurement processes, rather than ad hoc departmental purchasing, is directly correlated with cost savings. Increasing "managed spend" is one of the most reliable procurement improvement levers.
Moving from spreadsheet-based tracking to a unified spend analytics platform supports:
- Category-level benchmarking across sites
- Pricing trend identification before contract renewals
- Supplier consolidation opportunities across business units
- Maverick spend detection and reduction
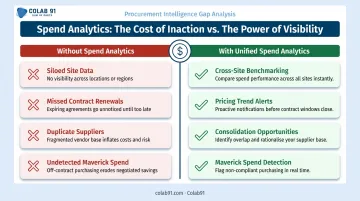
Without this infrastructure, procurement teams are negotiating individual contracts without knowing what the rest of the organization pays for the same categories.
Supplier Management: The Foundation for Quality and Cost Control
Qualification as a Formal Process
Supplier qualification in biopharma is a documented, auditable process - not a checklist. ICH Q10 requires qualification to happen before a purchase order is issued and remain reviewable throughout the relationship. A complete qualification package covers:
- GMP certification verification
- Site audit results
- Quality management system review
- Financial stability assessment
- Delivery performance history
Once qualified, suppliers don't stay qualified indefinitely. ISPE puts the standard re-audit interval for non-GMP key raw material suppliers at every 3–5 years; GMP-critical suppliers warrant shorter cycles.
Four-Tier Supplier Segmentation
Allocating relationship management resources appropriately requires segmenting suppliers by strategic importance:
| Tier | Description | Management Approach |
|---|---|---|
| Enterprise | Critical to multiple programs, high switching cost | Senior leadership engagement, joint development agreements |
| Strategic | Important to specific programs, limited alternatives | Category manager ownership, quarterly reviews |
| Core | Standard suppliers, multiple alternatives | Standardized contracts, semi-annual performance review |
| Extended Core | Transactional, easily replaceable | Catalog ordering, automated compliance checks |
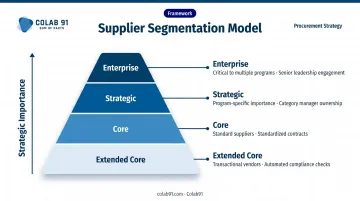
This framework - drawn from BCG's pharma TechOps research - prevents over-investing in transactional vendors while directing senior engagement, joint planning, and dedicated category ownership toward the suppliers that can actually derail a program.
Supplier Performance Monitoring
PDA research confirms that leading pharma companies embed quality metrics directly into supplier contracts, tying performance to measurable outcomes. Effective KPIs include:
- On-time delivery rate
- Right-first-time quality rate
- CAPA effectiveness and responsiveness
- Deviation frequency
Performance results should trigger formal reviews on a quarterly or semi-annual cycle. When a supplier falls below defined thresholds, that gap must activate a documented escalation path and contingency sourcing protocol - not an informal conversation that leaves no audit trail.
Building Scalable Procurement Capabilities for Long-Term Value
Sustainable procurement transformation in biopharma requires three investments made in parallel: people with category management and analytics skills, systems that provide real-time spend visibility, and analytics tools that convert raw procurement data into actionable insights.
The Mid-Market Challenge
Mid-market and PE-backed biopharma companies face a specific version of this problem. They need sophisticated procurement capability - spend analytics, supplier risk monitoring, category-level negotiation support - but they don't have the headcount or budget to build a large in-house team.
Offshore capability centers in India offer a practical answer. KPMG's 2026 analysis of healthcare and life sciences GCCs in India reports 150+ distinct HCLS GCCs, over 300,000 professionals, and operating cost reductions of up to 45% through AI and supply chain analytics. One research-driven pharma company cited in the report reduced purchase-requisition-to-PO turnaround time by 60% using AI automation in its India capability center.
These results reflect what's possible when offshore teams are built with domain depth, not just cost arbitrage in mind. Colab91 builds India-based procurement and analytics teams specifically for mid-market and PE-backed companies. The leadership team previously scaled Impendi's India operations to 100+ practitioners, serving PE clients including Carlyle Group, TPG, and BC Partners alongside healthcare clients like Kindred Healthcare and Amneal.
Their model covers:
- Spend analytics and savings opportunity assessment
- Supplier risk management and monitoring
- Strategic sourcing support across key categories
- Dedicated offshore teams operating as strategic hubs, not transactional delivery centers
The Self-Funding Model
Procurement transformation doesn't have to require large upfront capital. The sequencing matters:
- Start with spend visibility - Indirect spend consolidation generates early savings with minimal regulatory risk
- Reinvest early wins - Those savings fund analytics investments and deeper category management work
- Build sustainably - Mature category management and supplier programs fund ongoing capability building

This creates a self-funding cycle where transformation pays for itself rather than competing for budget against core R&D and manufacturing priorities.
Frequently Asked Questions
What are the 5 P's of procurement?
The 5 P's are People, Process, Product, Price, and Place. In biopharma, each carries extra weight: Product includes regulatory and quality status, Place flags geographic concentration risk, and Price means total cost of ownership - not just unit price.
What are the 7 stages of the procurement cycle?
The seven stages are: needs identification, supplier sourcing, supplier evaluation, negotiation and contracting, purchase order issuance, receipt and inspection, and payment/performance review. Biopharma layers GMP compliance checkpoints throughout, with the heaviest scrutiny applied at evaluation, inspection, and performance review.
What are the 10 C's of procurement?
Carter's 10 C's is a supplier evaluation framework covering dimensions from cost and capacity to culture and communication. In biopharma, two C's dominate: Clean (regulatory and environmental compliance) and Control (quality management systems), both of which drive supplier qualification decisions and audit outcomes.
What is the biggest procurement challenge in biopharma?
Balancing cost pressure with regulatory constraints that make supplier switching expensive and slow. This tension is compounded by decentralized purchasing across research, manufacturing, and clinical teams , which limits spend visibility and reduces negotiating leverage with vendors.
How can biopharma companies reduce procurement costs without compromising compliance?
The most accessible lever is indirect spend consolidation, which carries no regulatory change risk. Beyond that, better spend analytics increases the proportion of managed spend that generates consistent savings. Strategic supplier segmentation concentrates negotiation resources on high-value categories where the effort-to-savings ratio is highest.
What is category management in pharmaceutical procurement?
Category management groups related spend (APIs, CRO services, packaging, indirect spend) into strategic segments managed with tailored sourcing approaches. It allows procurement to prioritize opportunities by both savings potential and regulatory complexity, rather than reacting to individual purchase requests as they arise.